
 Pediatric cardiology involves the study of the heart and its function in infants, children and adolescents, including heart disease and congenital heart defects. Our specialist is located at Montana Children’s Specialists, a department of Kalispell Regional Medical Center.
Pediatric cardiology involves the study of the heart and its function in infants, children and adolescents, including heart disease and congenital heart defects. Our specialist is located at Montana Children’s Specialists, a department of Kalispell Regional Medical Center.
Patients
- Prenatal through age 25
Conditions Treated
- Autonomic dysfunction
- Cardiomyopathy
- Congenital heart disease
- Fetal cardiac evaluation
- Fetal rhythm abnormalities
- Heart murmurs
- Heart rhythm abnormalities
- Hypertension
- Hyperlipidemia
- Kawasaki disease
- Postural orthostatic tachycardia syndrome (POTS)
- Pulmonary hypertension
Services and Procedures
- 24-hour heart monitors
- Echocardiography
- Electrocardiography
- Event monitors
- Fetal echocardiography
- Pediatric exercise testing
What to Expect
Your Office Visit
Our team is trained in caring for young patients, and our goal is to make your visit as stress-free as possible.
Preparing for your visit:
- If your child is a new patient, you will receive a new patient packet. Please complete the packet and bring it to your visit.
- Please arrive 10-15 minutes early.
Be sure to bring:
- Identification, such as a drivers license
- Insurance card
- Proof of legal guardianship or medical power of attorney if anyone other than the custodial parent is bringing the child to the appointment
- List of your child’s medications
- Any medical records relating to your child’s condition
During your visit:
- Depending on the reason for your visit, an echocardiogram and electrocardiogram may be done.
- A nurse will review the packet with you and may ask for additional information.
- The nurse will weigh your child and take vitals including heart rate, temperature and blood pressure in an arm and a leg.
- You will then meet your medical provider, who will conduct an exam, carefully explain the necessary testing and treatment, and answer all your questions.
If you have any questions before or after your visit, call our office at (406) 257-8992.
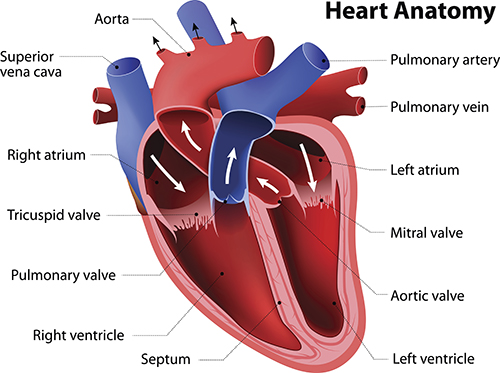
WHAT IS AN ECHOCARDIOGRAM?
- An echocardiogram (usually referred to as an echo) is an ultrasound of the heart. This imaging technique uses sound waves to create an image of the heart.
- An echocardiogram evaluates the anatomy of the heart, including the valves and walls, and can show any abnormalities, such as holes in the heart.
- An echocardiogram also demonstrates heart function, or how well the heart muscle squeezes and relaxes.
- An echocardiogram does not use radiation and is not painful or uncomfortable. The person who performs the echocardiogram has specialized training in heart anatomy and ultrasound. He or she will use ultrasound gel, which is necessary for transmission of sound waves.
- Most children have no trouble with echocardiograms. The study does require your child to be still for 20 to 30 minutes. We have movies and a calm atmosphere to support this. The most challenging ages are between 4 months and 3 years of age, and an echocardiogram can also be challenging for patients with developmental delays, sensory integration disorders or other special conditions.
- In rare cases, a complete echocardiogram is not possible because of the above challenges, and we will sometimes plan for your child to come back when he or she is older. If we decide with your family and your primary care provider that the echocardiogram should be done soon, we can schedule an echocardiogram with sedation. This is done at the hospital with an anesthesiologist.
WHAT IS AN ELECTROCARDIOGRAM?
- An electrocardiogram is also known as an EKG or ECG.
- This is a study of the electrical activity of the heart.
- An electrocardiogram involves 12 stickers on the chest for about one minute. The actual tracing only takes 10 seconds to complete.
- An electrocardiogram does not use radiation and does not cause pain or discomfort.
- Most children are able to have an electrocardiogram without sedation.
WHAT IS A HOLTER MONITOR?
- A Holter monitor is a 24-hour or 48-hour test of the electrical activity of the heart. Your child will wear the monitor under his or her clothing and it will not be visible. There are various options. Most have five stickers that attach to a small box with wires. The box is the size of a phone and can be clipped to clothing or kept in a pocket. Some insurance companies will cover a wireless monitor, which is easier to wear while playing sports.
- The reasons for using a Holter monitor include palpitations (feelings of the heart racing or going too slow, extra beats or skipped beats), fainting spells, chest pain, or to evaluate for abnormal rhythms in children with congenital heart disease or known rhythm abnormalities.
WHAT IS A 30-DAY MONITOR?
- A 30-day monitor is also known as an event monitor. This is a test of the electrical activity of the heart. Your child will wear the monitor under his or her clothing and it will not be visible. There are various options. Most have five stickers that attach to a small box with wires. The box is the size of a phone and can be clipped to clothing or kept in a pocket. Some insurance companies will cover a wireless monitor, which is easier to wear while playing sports.
- The reasons for a 30-day monitor include palpitations (feelings of the heart racing or going too slow, extra beats or skipped beats) and fainting spells that happen rarely and that would not likely be seen on a 24- or 48-hour monitor.
WHAT IS AN EXERCISE STUDY?
- An exercise study is also known as a stress test, cardiopulmonary exercise study or a treadmill test.
- This test is performed on a treadmill or a stationary bicycle, while we monitor your child’s heart rate, blood pressure, breathing, and degree of oxygen and carbon dioxide exchange.
- An exercise study may be indicated if your child has concerning symptoms with exercise, including chest pain, fainting, dizziness or palpitations. Children with congenital heart disease, abnormal heart muscle (cardiomyopathy) or known rhythm abnormalities often require an exercise study to evaluate whether they are safe to participate in strenuous activities such as sports, dance or other forms of exercise.
WHAT IS A CARDIAC CT SCAN?
- A CT (computed tomography) scan is a detailed scan of the heart.
- Occasionally, a CT scan is required to evaluate for abnormalities of the coronary arteries or the aorta.
- A CT scan does use radiation. This is minimized as much as possible for pediatric patients.
- Sometimes cardiac MRI (magnetic resonance imaging) is an alternative to CT.
- A benefit of cardiac CT over MRI is that it is much faster and usually does not require anesthesia or sedation.
WHAT IS A CARDIAC MRI?
- An MRI (magnetic resonance imaging) scan is a detailed scan of the heart.
- A cardiac MRI is used to evaluate the heart muscle and heart function, and can also be used to evaluate the aorta or pulmonary artery.
- An MRI does not use radiation.
- A cardiac MRI takes between 60 and 90 minutes, and requires a patient to be still and be able to follow directions.
- Children younger than 7 usually require sedation for a cardiac MRI. Between the ages of 7 and 10, we usually decide with the parents and the child whether they will require sedation. Children older than 10 can often complete a cardiac MRI without sedation.
WHAT IS AN ELECTROPHYSIOLOGY STUDY?
- An electrophysiology study is a procedure that is done at the hospital with anesthesia.
- During an electrophysiology study, a specialized cardiologist called an electrophysiologist uses catheters placed in leg veins to access the heart.
- An electrophysiology study may be performed for different reasons:
- Atrial fibrillation
- Supraventricular tachycardia
- Tetralogy of Fallot
- Ventricular tachycardia
- Wolff-Parkinson-White syndrome
- An electrophysiology study often includes an ablation, in which special catheters are used to treat an abnormal heart rhythm. These catheters may be hot (radiofrequency ablation) or cold (cryoablation).
WHAT IS A FETAL ECHOCARDIOGRAM?
- A fetal echocardiogram is an ultrasound of a baby’s heart prior to birth.
- Not every pregnant woman requires a fetal echocardiogram. The reasons for a fetal echocardiogram include:
- An abnormal 20-week anatomy scan
- Family history of congenital heart disease
- Concern about abnormal fetal heart rhythm
- Family history of abnormal heart rhythm in young people
- Mother with diabetes
- Mother with a rheumatologic disorder such as lupus, Sjögren’s syndrome, hypothyroidism, hyperthyroidism or rheumatoid arthritis
- Family history of trisomy 13, 18 or 21
- Other reasons may be determined by your obstetrician or perinatologist
- A fetal echocardiogram can be performed at Rocky Mountain Heart & Lung or Montana Perinatal Center.
WHAT IS A HEART CATHETERIZATION?
- A heart catheterization is a procedure that is done at the hospital with anesthesia.
- During a heart catheterization, a specialized cardiologist uses catheters placed in leg or arm veins or arteries to access the heart.
- A heart catheterization may be performed for different reasons:
- Aortic coarctation
- Atrial septal defect
- Patent ductus arteriosus
- Pulmonary hypertension
- A heart catheterization usually involves some radiation.
WHAT IS NUCLEAR IMAGING?
- Nuclear imaging is a type of radiology study that evaluates the function of the heart and the health of the heart muscle.
- This can also be called scintigraphy, SPECT or PET.
- This study may be ordered if your child has a history of congenital heart disease and is having trouble with exertion, if there are concerns about your child’s coronary arteries or for cardiomyopathy.
- A radiopharmaceutical tracer is given through a vein and undergoes spontaneous radioactive decay to emit radiation (usually gamma rays). The radiation is detected by external cameras to form images.
- This test does involve radiation.
WHAT ARE ORTHOSTATIC VITAL SIGNS?
- This is a simple test that can be done in any medical setting using a blood pressure cuff.
- Orthostatic vital signs are done by checking the blood pressure and heart rate in three positions: lying down, sitting and standing.
- This study is often done when someone has been fainting.
- Orthostatic vital signs can help in diagnosing types of autonomic dysfunction, including orthostatic intolerance, orthostatic hypotension, inappropriate sinus tachycardia and postural orthostatic tachycardia syndrome.
Conditions and Treatments
 ANOMALOUS AORTIC ORIGIN OF A CORONARY ARTERY
ANOMALOUS AORTIC ORIGIN OF A CORONARY ARTERY
What is anomalous aortic origin of a coronary artery?
The coronary arteries are two arteries that provide blood to the heart muscle. In a normal heart, the right coronary artery comes from the right coronary cusp of the aorta and the left coronary artery comes from the left coronary cusp. Rarely, the right coronary artery may come from the left cusp, or the left may come from the right cusp.
This can usually be diagnosed with an echocardiogram, but occasionally a cardiac CT scan may be needed.
How is it treated?
If your child has fainted with exercise or had chest pain with exercise, he or she should have surgery for an anomalous coronary artery. If this diagnosis is found incidentally, your cardiologist will discuss symptoms and may do an exercise study.
Currently most cardiologists and cardiac surgeons recommend surgery for a left coronary artery from a right coronary artery cusp. If your child has an anomalous right coronary artery from the left cusp, the current research is less clear. Usually this will be discussed with a group of cardiologists, who will make a decision together with your family.
AORTIC COARCTATION
What is aortic coarctation?
The aorta is the main artery that brings blood directly from the heart to the body. In rare cases, this artery can be too narrow. Sometimes the aorta is too narrow in one specific portion. Sometimes the aorta is too small in general.
When a baby is born, there is another large vessel, the patent ductus arteriosus, that also supplies blood flow to the body. This closes naturally in most babies. If it closes in a baby with an aortic coarctation, heart failure can happen.
How is it treated?
If a baby has a critical aortic coarctation, surgery is necessary. Older children may require surgery or a heart catheterization, depending on the child’s age and the degree of narrowing. In mild or moderate cases of aortic coarctation, children can be monitored over time.
Sometimes children with aortic coarctations have high blood pressure, even after the coarctation is repaired. Your child may require antihypertensive medications before and after surgery or catheterization.
AORTIC DILATION
What is aortic dilation?
The aorta is the main artery that brings blood directly from the heart to the body. Aortic dilation in children is defined by an aortic diameter that is at least two standard deviations above the mean for a given body surface area. The aorta can be dilated just after the valve (aortic root dilation) or it can be dilated in the ascending portion (ascending aortic dilation). Rarely, children can have abdominal aortic dilation.
There are a variety of causes of aortic dilation. People with connective tissue disorders are at higher risk for aortic dilation, especially those with Marfan syndrome or Loeys-Dietz syndrome. Some people with Ehlers-Danlos syndrome are also at risk. People with bicuspid aortic valves also can have aortic dilation. Some children have dilation for unknown reasons.
How is it treated?
Children with aortic dilation should be seen by a pediatric cardiologist. If your child has aortic dilation, it is important to talk with family about any other people with this problem, or anyone who may have Marfan syndrome, Loeys-Dietz syndrome, Ehlers-Danlos syndrome or other genetic syndromes. It is also important to ask family if anyone has had an aortic dissection, aortic aneurysm or aortic rupture.
Many children with aortic dilation will not require any intervention until they are adults, and some will never require intervention. In some cases, a medication may be recommended that could slow the rate of dilation. Depending on your child’s specific situation, restrictions from some sports may be necessary to avoid worsening of the aortic dilation.
In some cases, children with aortic dilation require surgery in order to avoid aortic dissection or aortic rupture, or to avoid damage to the aortic valve.
AORTIC MEMBRANE
See Subaortic Membrane
AORTIC REGURGITATION
What is aortic regurgitation?
The aortic valve is the valve between the left ventricle and the aorta. This is the valve that opens when the heart pumps blood out to the body. The aortic valve normally does not leak at all.
Aortic regurgitation is abnormal leaking of the aortic valve. This can be present at birth or develop over time. The most common cause of aortic regurgitation is a bicuspid aortic valve.
How is it treated?
If your child has aortic regurgitation, an echocardiogram will be done to evaluate whether the leaking is mild, moderate or severe. An exercise study may also be needed. Your cardiologist will discuss any symptoms your child may have, including chest pain, dizziness, fainting or palpitations.
If the leaking is severe, if the exercise study is abnormal or if your child has symptoms, he or she may need surgery.
AORTIC STENOSIS
What is aortic stenosis?
The aortic valve is the valve between the left ventricle and the aorta. This is the valve that opens when the heart pumps blood out to the body. Aortic stenosis is an abnormal narrowing of the valve. This can be present at birth or develop over time. The most common cause of aortic stenosis is a bicuspid aortic valve.
How is it treated?
If your child has aortic stenosis, an echocardiogram will be done to evaluate whether the narrowing is mild, moderate or severe. An exercise study may also be needed. Your cardiologist will discuss any symptoms your child may have, including chest pain, dizziness, fainting or palpitations.
If the aortic stenosis is severe, if the exercise study is abnormal or if your child has symptoms, the treatment is surgery or a heart catheterization.
AORTOPATHY
See Aortic Dilation
ARRHYTHMIA
What is an arrhythmia?
An arrhythmia is an irregular or abnormal heart rhythm, when the electrical impulses that control the heart are disrupted. The heart rate may be too fast or too slow, or it may have extra beats.
Examples include:
- Atrial ectopic tachycardia
- Atrial fibrillation
- Atrial flutter
- Brugada syndrome
- Junctional ectopic tachycardia
- Junctional rhythm
- Long QT syndrome
- Premature atrial contractions
- Premature ventricular contractions
- Sinus arrhythmia
- Sinus bradycardia
- Sinus tachycardia
- Supraventricular tachycardia
- Ventricular tachycardia
- Wolff-Parkinson-White syndrome
How is it treated?
Some arrhythmias in children do not require treatment, such as premature atrial contractions, bradycardia (if there are no symptoms) and rare premature ventricular contractions. Some arrhythmias can be controlled with lifestyle changes, including decreasing refined sugar intake, minimizing caffeine and minimizing stress. Some arrhythmias require medications.
For certain arrhythmias, an electrophysiology study is the best choice. An electrophysiology study is done in a catheterization laboratory with anesthesia and a specialized cardiologist known as an electrophysiologist. This study can be done to diagnose the exact arrhythmia and also to treat the arrhythmia with ablation.
Ablation may be done with radiofrequency energy (heat) or with cryoablation (cold), depending on where the problem is in the heart.
ATRIAL SEPTAL DEFECT
What is an atrial septal defect?
An atrial septal defect is a hole between the top two chambers of the heart (between the right atrium and the left atrium).
How is it treated?
Small atrial septal defects usually do not require treatment. A moderate-sized or large atrial septal defect will likely require treatment at some point. The treatment options include heart catheterization and surgery. The decision between these two options depends on your child’s age and size, the size of the defect, and any other heart abnormalities or medical conditions.
ATRIOVENTRICULAR SEPTAL DEFECT
What is an atrioventricular septal defect?
An atrioventricular septal defect is also known as an atrioventricular canal defect or an endocardial cushion defect. This is a combination of a hole between the right atrium and left atrium and a hole between the right and left ventricles. In this condition, the tricuspid and mitral valves are usually abnormal also. This is usually diagnosed before birth or in the first year.
How is it treated?
An atrioventricular septal defect usually requires heart surgery. In many cases this surgery should be done between 4 and 6 months of age. In mild cases, surgery can happen later.
AUTONOMIC DYSFUNCTION
What is autonomic dysfunction?
Autonomic dysfunction refers to a group of disorders in which the parasympathetic and sympathetic nervous systems are thought to be out of balance. In these cases, people may faint or feel like they are going to faint multiple times daily.
There are multiple types of autonomic dysfunction:
- Orthostatic intolerance
- Orthostatic hypotension
- Inappropriate sinus tachycardia
- Postural orthostatic tachycardia syndrome
How is it treated?
Many people with autonomic dysfunction can be treated with lifestyle modifications, including eating healthy, exercising regularly, minimizing screen time and staying involved in activities.
In some cases, lifestyle interventions should be accompanied by medications or other interventions such as biofeedback, counseling and complementary medicine.
In certain cases, treatment at a specialized treatment center may be recommended.
Learn More
dysautonomiainternational.org
BACTERIAL ENDOCARDITIS
What is bacterial endocarditis?
Bacterial endocarditis is an infection of the endocardium, which is the inner lining of the heart. Usually this is an infection of one or more heart valves. Rarely, an infection can occur where a hole is, or where a hole was fixed with surgery or heart catheterization. Endocarditis is extremely rare in children.
Bacteria can enter the bloodstream during a dental procedure, a tonsillectomy or adenoidectomy, an examination of the respiratory tract known as a rigid bronchoscopy, or a surgery on the respiratory tract, the gastrointestinal tract or the urinary tract.
Who is at risk for bacterial endocarditis?
- Children with congenital heart disease
- Children with artificial heart valves
- Children with a previous history of endocarditis
- Children who have had a heart transplant and have heart valve abnormalities
- Children or adolescents who use intravenous drugs
Sometimes, doctors recommend antibiotics prior to dental procedures for children at high risk for bacterial endocarditis. However, this is usually only for heart conditions associated with the highest risk of complications from endocarditis. The guidelines for this were updated by the American Heart Association in 2007. This should be discussed with your child’s health care provider and primary care doctor.
How is it prevented?
Oral hygiene is essential to avoid endocarditis, especially in children who are at risk. Your child should have regular visits to the dentist at least every six months. Your child should brush twice daily and floss at least once daily. Usually children under age 5 require help with brushing and flossing. In some cases endocarditis is unavoidable.
How is it treated?
Antibiotics are required to treat bacterial endocarditis. Sometimes surgery is necessary for repair or replacement of a valve.
If endocarditis occurs near an atrial septal defect or a ventricular septal defect, this will likely require closure after the infection is treated.
BICUSPID AORTIC VALVE
What is a bicuspid aortic valve?
The aortic valve is the valve between the left ventricle and the aorta. This is the valve that opens when the heart pumps blood out to the body. The aortic valve normally has three leaflets and looks like the Mercedes symbol when it is closed.
People with bicuspid aortic valves only have two aortic valve leaflets. This is the most common type of congenital heart disease.
A bicuspid aortic valve is often diagnosed during a medical provider’s physical exam. Sometimes it is diagnosed incidentally when an echocardiogram is being done for another reason.
Some people with bicuspid aortic valves never have any problems with the valve. In some cases, these valves do not function well over time. People with bicuspid aortic valves can develop aortic stenosis, aortic regurgitation or aortic dilation.
How is it treated?
In many cases, people with bicuspid aortic valves do not require any treatment. In other cases, if there is aortic stenosis, aortic regurgitation or aortic dilation, they may require medications, heart catheterization or surgery.
Bicuspid aortic valves run in families and are often genetic. If one person in a family has a bicuspid aortic valve, all first-degree relatives should be screened. Genetic counseling is recommended in some cases.
CARDIAC ARRHYTHMIA
See Arrhythmia
CARDIOMYOPATHY
What is cardiomyopathy?
Cardiomyopathy is an abnormality of the muscle of the heart. This can be something a child is born with, or it can happen later. Some types of cardiomyopathy can be caused by viruses. Cardiomyopathy is extremely rare in children.
There are four main types of cardiomyopathy:
- Dilated cardiomyopathy
- Hypertrophic cardiomyopathy
- Left ventricular noncompaction cardiomyopathy
- Restrictive cardiomyopathy
How is it treated?
Cardiomyopathy can sometimes be treated with medications, including beta blockers, ACE inhibitors and diuretics. Sometimes children are restricted from sports for safety reasons. In cases of severe cardiomyopathy, some children require surgery or a heart transplant.
CHEST PAIN
What causes chest pain in children and adolescents?
Chest pain in children can be distressing for the child and the family. Fortunately, in most cases chest pain in children and adolescents is not caused by a heart problem.
The most common cause of chest pain in children and adolescents is chest wall pain. The chest wall includes the muscles and bones that protect the lungs and heart, including the ribs and sternum.
Other possible noncardiac causes of chest pain include:
- Anxiety
- Asthma
- Costochondritis (benign inflammation of the ribs)
- Gastroesophageal reflux
- Tietze syndrome (benign inflammation of one or more of the costal cartilages)
In some cases, chest pain in children can truly be from the heart. Some examples of this are:
- Aortic dissection
- Arrhythmia
- Coronary artery disease
- Coronary artery spasm
- Drug abuse (most commonly cocaine)
- Kawasaki disease
- Myocarditis
- Pericarditis
How is it treated?
The treatment of chest pain depends on the cause. Your child will be evaluated for chest pain. Evaluation will always include a detailed history and physical. Other tests may be required, including an electrocardiogram, echocardiogram and possibly an exercise study.
On rare occasions, your cardiologist may need a more detailed look at your child’s coronary arteries, with an advanced imaging study such as a cardiac CT scan, cardiac MRI, nuclear imaging or a heart catheterization.
If the chest pain does not seem to be caused by the heart, your child may have chest wall pain, asthma or gastroesophageal reflux. These are all treated differently. Chest wall pain is often treated with anti-inflammatory medications, asthma is treated with inhalers, and gastroesophageal reflux is treated with diet and lifestyle changes or with acid blockers.
CONGENITAL HEART DISEASE
What is congenital heart disease?
Congenital heart disease is any abnormality of the heart that is present at birth. This occurs in about 1 percent of total births in the United States. Congenital heart defects are the most common birth defects.
Types of congenital heart disease include:
- Bicuspid aortic valve
- Double inlet left ventricle
- Double outlet right ventricle
- Ebstein’s anomaly
- Hypoplastic left heart syndrome
- Partial anomalous pulmonary venous return
- Pulmonary atresia
- Pulmonary atresia with intact ventricular septum
- Pulmonary atresia with ventricular septal defect
- Subaortic membrane
- Tetralogy of Fallot
- Total anomalous pulmonary venous return
- Transposition of the great arteries
- Tricuspid atresia
- Truncus arteriosus
DILATED CARDIOMYOPATHY
What is dilated cardiomyopathy?
Dilated cardiomyopathy is the most common type of cardiomyopathy in children. This is an abnormality of the heart muscle in which the ventricles are abnormally enlarged and weak. Some children with dilated cardiomyopathy have no symptoms, and some develop heart failure (difficulty breathing, difficulty eating, sweating and problems growing).
Dilated cardiomyopathy can be caused by a virus. There is a type of dilated cardiomyopathy that runs in families. In many cases, there is no known reason for dilated cardiomyopathy.
How is it treated?
Dilated cardiomyopathy can sometimes be treated with medications, including beta blockers, ACE inhibitors and diuretics. Sometimes children are restricted from sports for safety reasons. In cases of severe cardiomyopathy, some children require surgery or a heart transplant.
DOUBLE INLET LEFT VENTRICLE
What is double inlet left ventricle?
In a normal heart, the tricuspid valve empties from the right atrium into the right ventricle and the mitral valve empties from the left atrium into the left ventricle. Double inlet left ventricle is a rare type of congenital heart disease in which both the tricuspid and mitral valves open into the left ventricle. There is also usually a ventricular septal defect. This is often diagnosed before birth or just after birth. Pulse oximetry screening in the newborn nursery can help diagnose this.
How is it treated?
Most children with double inlet left ventricle require heart surgery. In many cases, this will involve two or three operations before the child is 5 years old.
DOUBLE OUTLET RIGHT VENTRICLE
What is double outlet right ventricle?
In a normal heart, the pulmonary artery comes from the right ventricle and brings deoxygenated blood to the lungs, and the aorta comes from the left ventricle and brings oxygenated blood to the body. Double outlet right ventricle is a rare type of congenital heart disease in which both the pulmonary artery and the aorta come from the right ventricle. There is also usually a ventricular septal defect. This is often diagnosed before birth or just after birth. Pulse oximetry screening in the newborn nursery can help to diagnose this.
How is it treated?
Most children with double outlet right ventricle require heart surgery. In some cases, only one surgery is necessary in childhood; this is usually a closure of the ventricular septal defect. In other cases, especially if the left ventricle is significantly smaller than the right ventricle, the best thing is a palliative series of operations.
Children with double outlet right ventricle often require heart surgery again in adolescence or as adults.
EBSTEIN’S ANOMALY
What is Ebstein’s anomaly?
Ebstein’s anomaly is a congenital heart defect involving the tricuspid valve, which is the valve between the right atrium and the right ventricle. In this abnormality, the valve leaflets are lower than normal in the right ventricle. Often the valve leaks significantly, and this can cause the right atrium to become large.
Cases of severe Ebstein’s anomaly are often diagnosed before birth. In mild cases, diagnosis may occur later. Sometimes the first clue to this diagnosis is abnormal heart rhythms, most commonly supraventricular tachycardia.
How is it treated?
Children with Ebstein’s anomaly often require heart surgery. In mild cases, it may be safe to monitor the child over time.
ENDOCARDITIS
See Bacterial Endocarditis
FAINTING
What is fainting?
Fainting is also known as syncope. Fainting is a complete loss of consciousness. There is also a symptom called presyncope, which is the feeling of almost fainting. Fainting can be quite alarming to families and to the person who faints.
Fainting is usually not dangerous in children. The most common type of fainting is vasovagal (also known as neurocardiogenic or orthostatic). This type of fainting usually happens when blood flow to the head is temporarily inadequate, resulting in loss of consciousness. This may be due to standing up fast, locking knees while standing for a long time, standing in a hot environment, having ears cleaned or pierced, or having hair cut or styled.
Most children who faint will only faint once or twice. This commonly can occur in choir, standing in line, in church or in a hot cramped environment.
Some people faint more often. There is a group of problems called autonomic dysfunction, in which the parasympathetic and sympathetic nervous systems are thought to be out of balance. In these cases, people may faint or feel like they are going to faint multiple times daily.
In rare cases, fainting can be the sign of a dangerous heart problem. The following are reasons to seek care immediately:
- Fainting with exercise
- Fainting while lying down
- Requiring assistance to wake up after fainting
- Palpitations before fainting
- Fainting in any child who is already seen by a cardiologist for congenital heart disease or an arrhythmia
How is it treated?
Most people who faint can be treated by increasing their water intake. Growing children and teenagers may have “head rushes” that happen when they stand, and these are more common during and after growth spurts. This can usually be treated by standing up more slowly, by crouching down if they feel like they will faint (crouching down in a squatting position pushes a lot of blood up to the heart and then to the head), by drinking more water and by eating plenty of fruits and vegetables, which release water slowly to the body throughout the day.
In cases of autonomic dysfunction, medications may be recommended to decrease the frequency of fainting.
FETAL ARRHYTHMIA
What is a fetal arrhythmia?
A baby’s heart starts beating between two and three weeks after conception (about four or five weeks after your last menstrual period). A fetal arrhythmia is an abnormal heart rhythm in a baby’s heart before birth. The heart rate may be too fast or too slow, or it may have extra beats.
Your baby’s heart rate will be checked at most prenatal visits. A normal fetal heart rate depends on gestational age but is usually between 110 and 180 beats per minute. If there are concerns about your baby’s heart rate or rhythm, longer heart rate monitoring may be recommended.
In some cases, a fetal echocardiogram should be done to evaluate your baby’s heart rhythm.
How is it treated?
Most fetal arrhythmias do not require treatment. The most common type of fetal arrhythmia is premature atrial contractions. Other common types are supraventricular tachycardia and atrial flutter. These arrhythmias sometimes require treatment, which is usually medication given to the mother.
In rare cases, a baby’s heart rate is too slow. If this is diagnosed quickly, there are medications that may be effective. This is more common in congenital heart disease and in babies whose mothers have a rheumatologic disorder such as lupus, Sjögren’s syndrome, hypothyroidism or rheumatoid arthritis. It is important to inform your prenatal care provider of any medical history, especially any history of autoimmune disorders.
HEART FAILURE
What is heart failure?
Heart failure is a general term to describe the heart’s inability to supply adequate oxygenated blood to the body. There are multiple types of heart failure in children, and all are rare.
Heart failure can result from an abnormality of the heart muscle. See cardiomyopathy for details.
Heart failure can also refer to a situation in which there is more blood flow through the lungs than through the body. The cause of this is usually a ventricular septal defect, atrial septal defect, patent ductus arteriosus or other type of congenital heart disease.
How is it treated?
Heart failure can sometimes be treated with medications, including beta blockers, ACE inhibitors and diuretics. Sometimes children are restricted from sports for safety reasons. If the heart failure is caused by congenital heart disease, the treatment is usually surgical or interventional repair of the defect.
In cases of severe heart failure due to cardiomyopathy, some children require a heart transplant.
HEART MURMUR
What is a heart murmur?
A heart murmur is a sound that can be heard with a stethoscope. In children and young adults, heart murmurs are common and are often benign. Children with strong hearts and small chests often have sounds heard that would not be heard in adults, and usually these are sounds that indicate a healthy heart. Benign murmurs become louder when a child is excited or has a fever.
In some cases, a heart murmur is a sign of a heart abnormality. Your primary care provider will listen to your child’s heart at every visit. Some heart murmurs are always benign, and your primary care provider will reassure you if they hear one of those. In some cases, your primary care provider may hear a murmur that requires further evaluation. Your provider may refer your child for a cardiology visit or an echocardiogram.
How is it treated?
Many heart murmurs are benign. If your child is referred to a pediatric cardiologist, the murmur may still be found to be benign. Rarely, a murmur is a sign of congenital heart disease or another heart abnormality.
Common causes of pathologic murmurs are aortic stenosis, aortic regurgitation, atrial septal defect, patent ductus arteriosus, pulmonary stenosis, pulmonary regurgitation and ventricular septal defect. In those cases, treatment depends on the specific problem.
HYPERTROPHIC CARDIOMYOPATHY
What is hypertrophic cardiomyopathy?
Hypertrophic cardiomyopathy occurs when the walls of the heart become unusually thick. This can affect the heart’s ability to pump blood effectively, especially during exercise. This type of cardiomyopathy can also cause abnormal heart rhythms, which can lead to sudden death.
Hypertrophic cardiomyopathy is often genetic, and if one person in a family has hypertrophic cardiomyopathy, all first-degree relatives should be screened. Genetic counseling is often recommended.
How is it treated?
Hypertrophic cardiomyopathy can sometimes be treated with medications, including beta blockers, ACE inhibitors and diuretics. Sometimes children are restricted from sports for safety reasons. In cases of severe cardiomyopathy, some children require surgery or a heart transplant.
HYPOPLASTIC LEFT HEART SYNDROME
What is hypoplastic left heart syndrome?
Hypoplastic left heart syndrome is a type of severe congenital heart disease. In this defect, the left ventricle is too small to pump blood effectively to the body. The aorta and mitral valve are also small. There is often an aortic coarctation.
This is often diagnosed before birth or just after birth. Pulse oximetry screening in the newborn nursery can help to diagnose this.
How is it treated?
Most children with hypoplastic left heart syndrome require heart surgery. The most common treatment is a palliative series of operations. This usually consists of at least three heart surgeries in early childhood. In some cases, a heart transplant is a better option.
INAPPROPRIATE SINUS TACHYCARDIA
What is inappropriate sinus tachycardia?
Inappropriate sinus tachycardia is a type of autonomic dysfunction, defined by a heart rate that is consistently faster than the body requires. This may cause a sensation of palpitations, or a racing heart. Your child’s doctor may use a cardiac monitor (a Holter monitor or event monitor) to learn more about the heart rhythm.
How is it treated?
Many people with inappropriate sinus tachycardia can be treated with lifestyle modifications, including eating healthy, exercising regularly, minimizing screen time and staying involved in activities.
In some cases, lifestyle interventions should be accompanied by medications or other interventions such as biofeedback, counseling and complementary medicine.
Learn More
dysautonomiainternational.org
INTERRUPTED AORTIC ARCH
What is an interrupted aortic arch?
The aorta is the main artery that brings blood directly from the heart to the body. In rare cases, this artery can be completely closed, which is called an interruption. This is considered the most extreme form of aortic coarctation.
When a baby is born, there is another large vessel, the patent ductus arteriosus, that also supplies blood flow to the body. This closes naturally in most babies. If it closes in a baby with an interrupted aortic arch, heart failure can happen quickly.
An interrupted aortic arch is often diagnosed before birth or just after birth. Pulse oximetry screening in the newborn nursery can help diagnose this.
How is it treated?
If a baby has an interrupted aortic arch, heart surgery is necessary. Sometimes children with an interrupted aortic arch have high blood pressure, even after the arch is repaired. Your child may require antihypertensive medications after surgery.
Children with an interrupted aortic arch often require another heart surgery or heart catheterization later in life.
KAWASAKI DISEASE
What is Kawasaki disease?
Kawasaki disease is a problem in which blood vessels throughout the body become inflamed. All children with Kawasaki disease have at least five days of high fever, often above 104 degrees Fahrenheit.
There are five additional criteria for typical Kawasaki disease:
- Redness of the mouth or cracked lips
- Rash
- Swelling or redness of the hands or feet
- Red eyes (conjunctivitis)
- Swollen lymph nodes in the neck
Kawasaki is most common in children between the ages of 6 months and 6 years. Rarely, it occurs in younger or older patients. Kawasaki disease can be challenging to diagnose, as the criteria are not always seen at the same time, and there are viral infections that can have similar symptoms. Your doctor may take a blood test to check for other possible signs of Kawasaki disease. An echocardiogram can sometimes help in the diagnosis of atypical Kawasaki disease.
If your child is diagnosed with Kawasaki disease, an echocardiogram is necessary to evaluate the coronary arteries. The coronary arteries are two small arteries that provide the heart muscle with blood. Kawasaki disease can cause dilation of these arteries, which over many years can lead to early serious coronary artery disease. This is the main reason why it is important to diagnose and treat Kawasaki disease.
How is it treated?
Children with Kawasaki disease are admitted to a hospital for treatment. The current recommended treatment for Kawasaki disease is one dose of intravenous immunoglobulin and high-dose aspirin. If this treatment is successful in decreasing inflammation, the child can go home with low-dose aspirin for at least six to eight weeks. If there is still inflammation, there are other treatments that have been shown to be effective.
An echocardiogram should be done at the time of diagnosis, one to two weeks after diagnosis and six to eight weeks after diagnosis. If any of these echocardiograms show dilation of the coronary arteries, other medications may be required.
All children who have had Kawasaki disease should be seen by a cardiologist at least every five years, even as adults. The reason for this is that even people who had no coronary artery dilation have been seen in studies to have abnormal coronary arteries later in life.
It is extremely important for any person with a history of Kawasaki disease to have a healthy lifestyle.
LEFT VENTRICULAR NONCOMPACTION CARDIOMYOPATHY
What is left ventricular noncompaction cardiomyopathy?
The left ventricle is the muscular chamber that pumps blood to the body. A normal left ventricle has a smooth wall. In patients with left ventricular noncompaction, the left ventricular wall is coarse instead of smooth. This type of cardiomyopathy is the most recently discovered, and less is known about it than about the other types of cardiomyopathy.
Left ventricular noncompaction can be associated with a genetic syndrome or can be diagnosed along with any other type of cardiomyopathy (dilated, hypertrophic or restrictive). It also can occur on its own with no identifiable cause. Because left ventricular noncompaction is often genetic, if one person in a family has it, all first-degree relatives should be screened. Genetic counseling is often recommended.
Some children with left ventricular noncompaction have symptoms of heart failure, such as difficulty breathing, difficulty eating, sweating and problems growing. Some have no symptoms. If your child is diagnosed with or suspected to have left ventricular noncompaction, your doctor may discuss other tests with you, including a cardiac MRI and a Holter monitor.
How is it treated?
Left ventricular noncompaction cardiomyopathy can sometimes be treated with medications, including beta blockers, ACE inhibitors and diuretics. Sometimes children are restricted from sports for safety reasons.
In cases of severe cardiomyopathy, some children require surgery or a heart transplant.
LONG QT SYNDROME
What is long QT syndrome?
The QT interval is a part of an electrocardiogram. Long QT syndrome is a genetic disorder in which the QT interval on the electrocardiogram is longer than normal. People with this syndrome have an increased risk of dangerous heart rhythms.
People with genetic long QT syndrome are born with a mutation. Certain medications can also cause a QT interval to be long in someone without long QT syndrome. These medications can be dangerous for people with genetic long QT syndrome.
How is it treated?
Long QT syndrome is treatable. Many patients with long QT are given beta blocker medications. In some cases, surgery or an implantable device is necessary. It is important to avoid medications known to prolong the QT interval.
Learn More
crediblemeds.org
MARFAN SYNDROME
What is Marfan syndrome?
Marfan syndrome is a genetic disorder that affects the body’s connective tissue. Connective tissue is made up of proteins. The specific protein that is affected in Marfan syndrome is fibrillin-1. People with Marfan syndrome have a mutation in the gene that tells the body how to make fibrillin-1. This can cause problems in connective tissues throughout the body.
The most common heart problems in people with Marfan syndrome are aortic dilation and mitral valve prolapse.
How is it treated?
If a child already has a diagnosis of Marfan syndrome, he or she should see a cardiologist. Marfan syndrome involves other parts of the body, including the eyes, bones, joints and other blood vessels.
If there is a suspicion of Marfan syndrome, your child’s primary care doctor may calculate a systemic score or refer to a cardiologist for further evaluation.
Sometimes Marfan syndrome is suspected during an eye exam with an ophthalmologist or optometrist. People with Marfan syndrome often have severe myopia (nearsightedness) or eye lens dislocation.
A cardiologist may recommend a medication such as a beta blocker, ACE inhibitor or angiotensin receptor blocker. These medications are used to decrease the rate of aortic dilation. People with Marfan syndrome are often restricted from some sports, especially isometric sports.
If aortic dilation becomes severe, a person with Marfan syndrome may require surgery.
Learn More
marfan.org
MITRAL REGURGITATION
What is mitral regurgitation?
The mitral valve is the valve between the left atrium and the left ventricle. The mitral valve normally either does not leak at all or leaks a trivial amount. Mitral regurgitation is abnormal leaking of the mitral valve. This can be present at birth or develop over time. The most common cause of mitral regurgitation is mitral valve prolapse. Mitral regurgitation also can be caused by rheumatic heart disease. People with cardiomyopathy also may have mitral regurgitation.
How is it treated?
If your child has mitral regurgitation, an echocardiogram will be done to determine whether the leaking is mild, moderate or severe. Your cardiologist will discuss any symptoms your child may have, including chest pain, dizziness, fainting or palpitations.
If the leaking is severe, if other parts of the heart are changing as a result of the regurgitation or if your child has symptoms, your child may require surgery.
MITRAL STENOSIS
What is mitral stenosis?
The mitral valve is the valve between the left atrium and the left ventricle. Mitral stenosis is an abnormal narrowing of the valve. This can be present at birth or develop over time. Mitral stenosis can be caused by rheumatic heart disease.
How is it treated?
If your child has mitral stenosis, an echocardiogram will be done to evaluate whether the narrowing is mild, moderate or severe. An exercise study also may be needed. Your cardiologist will discuss any symptoms your child may have, including chest pain, dizziness, fainting or palpitations.
If the narrowing is severe, if the exercise study is abnormal or if your child has symptoms, the treatment is surgery or a heart catheterization.
MITRAL VALVE PROLAPSE
What is mitral valve prolapse?
The mitral valve is the valve between the left atrium and the left ventricle. Mitral valve prolapse is a condition in which the two leaflets of the mitral valve do not close normally and instead protrude (prolapse) in the opposite direction, into the left atrium. In most cases, especially when mitral valve prolapse is mild, this does not cause problems.
The most common cause of mitral valve prolapse is abnormally flexible mitral valve leaflets (this is called myxomatous valve disease). In rare cases, mitral valve prolapse is part of a more general medical condition called a connective tissue disorder.
How is it treated?
If your child has mitral valve prolapse, an echocardiogram will be done to evaluate whether the prolapse is mild, moderate or severe and whether there is any mitral regurgitation. Your cardiologist will discuss any symptoms your child may have, including chest pain, dizziness, fainting or palpitations. Usually, mitral valve prolapse does not require treatment.
Rarely, if a person has abnormal heart rhythms, or if there is mitral regurgitation or other changes in the heart, surgery or a heart catheterization may be recommended.
MURMUR
See Heart Murmur
MYOCARDITIS
What is myocarditis?
Myocarditis is an infection or inflammation of the myocardium, which is the middle muscular layer of the heart wall. Usually myocarditis is caused by a viral infection. Symptoms of myocarditis include chest pain, decreased energy, abdominal pain and palpitations (feelings of the heart racing).
Myocarditis can be mild, but it also can be severe and life-threatening. Myocarditis is extremely rare in children.
How is it treated?
Mild myocarditis requires rest and supportive care (fluids, diuretics and sometimes a hospital stay). If myocarditis is severe, a hospital stay is necessary. Severe myocarditis may sometimes be treated with medications including ACE inhibitors and diuretics.
In cases of severe heart failure due to myocarditis, some children require a heart transplant.
ORTHOSTATIC HYPOTENSION
What is orthostatic hypotension?
Orthostatic hypotension is a type of autonomic dysfunction. It is also known as postural hypotension (low blood pressure when standing). The symptoms include lightheadedness, feeling like fainting or actually fainting.
Your doctor may perform a simple test called orthostatic vital signs. The definition of orthostatic hypotension is a decrease in systolic blood pressure of at least 20 mmHg or a decrease in diastolic blood pressure of at least 10 mmHg within three minutes of standing.
How is it treated?
Many people with orthostatic hypotension can be treated with lifestyle modifications, including an increase in fluid intake, fruits and vegetables. Whole fruits and vegetables are important, as they are digested slowly and release water gradually throughout the day, so there is a consistent amount of water in the body.
Regular exercise also helps with orthostatic hypotension by strengthening the leg muscles and increasing the tone in the leg veins, which increases return of blood to the heart. Compression stockings also can decrease pooling of blood in the legs and increase return to the heart.
People who know they have orthostatic hypotension can train themselves to get up slowly and gradually, and to keep their legs moving when they are standing for a long time or feeling lightheaded.
In some cases, lifestyle interventions should be accompanied by medications or other interventions such as biofeedback, counseling and complementary medicine.
Learn More
dysautonomiainternational.org
ORTHOSTATIC INTOLERANCE
What is orthostatic intolerance?
Orthostatic intolerance is a type of autonomic dysfunction. The symptoms usually occur when standing and include lightheadedness, palpitations (feelings of the heart racing), nausea, malaise, feeling like fainting or actually fainting.
Your doctor may perform a simple test called orthostatic vital signs. People who have orthostatic intolerance with a significant change in heart rate on standing, without orthostatic hypotension, sometimes have postural orthostatic tachycardia syndrome.
How is it treated?
Many people with orthostatic intolerance can be treated with lifestyle modifications, including eating healthy, exercising regularly, minimizing screen time and staying involved in activities.
In some cases, lifestyle interventions should be accompanied by medications or other interventions such as biofeedback, counseling and complementary medicine.
In rare cases, treatment at a specialized treatment center may be recommended.
Learn More
dysautonomiainternational.org
PARTIAL ANOMALOUS PULMONARY VENOUS RETURN
What is partial anomalous pulmonary venous return?
Partial anomalous pulmonary venous return is a type of congenital heart disease.
In a normal heart, there are four pulmonary veins (two from the right lung and two from the left lung) that bring oxygenated blood back from the lungs to the left atrium, so that the oxygenated blood can be pumped out into the body.
In children with partial anomalous pulmonary venous return, one or more (but not all four) of the pulmonary veins return to the wrong place. There are multiple types of partial anomalous pulmonary venous return.
How is it treated?
Some children with partial anomalous pulmonary venous return do not require any treatment. In some cases, heart surgery is recommended. Children with this condition should always be seen by a cardiologist.
PATENT DUCTUS ARTERIOSUS
What is a patent ductus arteriosus?
A patent ductus arteriosus is also known as a patent arterial duct. The arterial duct is an artery that is as big as the aorta before birth. This is necessary for fetal circulation while the baby is attached to the placenta. Normally, this closes in the first few days after birth. In some cases, the duct does not close, and this is called a patent ductus arteriosus. It is an unnecessary opening between the aorta and the pulmonary artery. This is more common in premature babies and in babies with trisomy 21.
In most cases, patent ductus arteriosus is small and does not cause any problems or symptoms.
How is it treated?
Children with a patent ductus arteriosus that is still present two weeks after birth should see a cardiologist. A cardiologist will use an echocardiogram to evaluate the size of the problem and whether it is affecting any other parts of the heart.
Patent ductus arteriosus may never cause symptoms. However, there is a tiny risk of bacterial endocarditis, so if your medical provider or cardiologist can hear the patent ductus arteriosus when listening to the heart with a stethoscope, the current recommendations are to close the duct.
Closure of a patent ductus arteriosus can often be done with a heart catheterization. In rare cases, surgery may be needed.
PERICARDITIS
What is pericarditis?
Pericarditis is an inflammation or infection of the pericardium, which is the thin saclike membrane surrounding the heart. Pericarditis often occurs during or after a viral infection.
The most common symptom of pericarditis is chest pain behind the breastbone or in the left side of the chest. The pain often worsens with a deep breath or when lying down. Sitting up and leaning forward often lessens the pain. Most commonly, pericarditis lasts less than two weeks, but occasionally it can last longer.
An electrocardiogram and an echocardiogram may be used to diagnose pericarditis.
How is it treated?
Pericarditis is often relieved with ibuprofen or naproxen. For most people, these are the only medications required. A medication called colchicine is used in some cases.
Pericarditis usually improves within a few weeks. Often, children are restricted from competitive sports while they are having symptoms of pericarditis.
POSTURAL ORTHOSTATIC TACHYCARDIA SYNDROME
What is postural orthostatic tachycardia syndrome?
Postural orthostatic tachycardia syndrome is a type of autonomic dysfunction. Symptoms include fatigue, lightheadedness, headache, palpitations (feelings of the heart racing), nausea, diminished concentration, shaking, fainting, chest pain and shortness of breath.
If your child is evaluated for this syndrome, your doctor may perform a simple test called orthostatic vital signs. Postural orthostatic tachycardia syndrome may be the diagnosis if there is a fast heart rate when standing accompanied by orthostatic intolerance, with the following criteria:
- A persistent increase of more than 30 beats per minute or an absolute heart rate of more than 120 beats per minute within 10 minutes of moving from lying down to standing
- Absence of orthostatic hypotension
Depending on the person’s symptoms, additional testing may be needed to evaluate for other medical problems.
How is it treated?
Many people with postural orthostatic tachycardia syndrome can be treated with lifestyle modifications, including eating healthy, exercising regularly, minimizing screen time and staying involved in activities.
In some cases, lifestyle interventions should be accompanied by medications or other interventions such as biofeedback, counseling and complementary medicine.
In rare cases, treatment at a specialized treatment center may be recommended.
Learn More
dysautonomiainternational.org
PREMATURE ATRIAL CONTRACTIONS
What are premature atrial contractions?
The heart’s electrical system prompts the heart to contract and efficiently pump blood to the lungs and body. These electrical impulses begin in the upper chambers of the heart (the atria).
Some people have extra beats that come from other parts of the upper chambers of the heart. These are premature atrial contractions. These can cause palpitations (feelings of the heart racing or skipping).
Most people with premature atrial contractions have otherwise normal hearts. If your child is diagnosed with premature atrial contractions, a heart monitor may be recommended in order to determine how many contractions occur in a day.
How are they treated?
Most people with premature atrial contractions do not require any treatment. Some lifestyle changes may decrease the amount of contractions, including decreasing refined sugar intake, minimizing caffeine and minimizing stress.
People with premature atrial contractions rarely require medications or other interventions.
PREMATURE VENTRICULAR CONTRACTIONS
What are premature ventricular contractions?
The heart’s electrical system prompts the heart to contract and efficiently pump blood to the lungs and body. These electrical impulses begin in the upper chambers of the heart.
Some people have extra beats that come from their heart’s lower chambers. These are premature ventricular contractions. These can cause palpitations (feelings of the heart racing).
Most people with premature ventricular contractions have otherwise normal hearts. If your child is diagnosed with premature ventricular contractions, a heart monitor may be recommended in order to determine how many contractions occur in a day.
How are they treated?
Most people with premature ventricular contractions do not require any treatment. Some lifestyle changes may decrease the amount of contractions, including decreasing refined sugar intake, minimizing caffeine and minimizing stress.
In some cases, medications may be recommended to decrease the amount of premature ventricular contractions.
In rare cases, an electrophysiology study is the best choice. An electrophysiology study is done in a catheterization laboratory with anesthesia and a specialized cardiologist known as an electrophysiologist. This study can be done to diagnose the exact arrhythmia and also to treat the arrhythmia with ablation. Ablation may be done with radiofrequency energy (heat) or with cryoablation (cold), depending on where the problem is in the heart.
PULMONARY ATRESIA
What is pulmonary atresia?
The pulmonary valve is the valve between the right ventricle and the pulmonary artery. This is the valve that opens when the right ventricle pumps deoxygenated blood to the lungs in order to be oxygenated. Pulmonary atresia is a type of congenital heart disease. In this defect, there is no pulmonary valve.
This is often diagnosed before birth or just after birth. Pulse oximetry screening in the newborn nursery can help to diagnose this.
There are two distinct types of pulmonary atresia:
PULMONARY ATRESIA WITH INTACT VENTRICULAR SEPTUM
What is pulmonary atresia with intact ventricular septum?
The pulmonary valve is the valve between the right ventricle and the pulmonary artery. This is the valve that opens when the right ventricle pumps deoxygenated blood to the lungs in order to be oxygenated.
Pulmonary atresia with intact ventricular septum is a type of congenital heart disease. In this defect, there is no pulmonary valve opening. The right ventricle is sometimes too small to function normally. In some cases, the right ventricle is an adequate size. The coronary arteries of the heart are often abnormal in this type of congenital heart disease.
How is it treated?
Most children with pulmonary atresia with intact ventricular septum require a heart catheterization or heart surgery. Often a heart catheterization is recommended to evaluate the coronary arteries. In some cases during catheterization, the valve may be opened.
Sometimes a pulmonary conduit may be placed surgically. In many cases a staged surgical approach is the best choice for this condition. This usually consists of at least three heart surgeries in early childhood.
In some cases, a heart transplant is a better option.
PULMONARY ATRESIA WITH VENTRICULAR SEPTAL DEFECT
What is pulmonary atresia with ventricular septal defect?
The pulmonary valve is the valve between the right ventricle and the pulmonary artery. This is the valve that opens when the right ventricle pumps deoxygenated blood to the lungs in order to be oxygenated.
Pulmonary atresia with a ventricular septal defect is a type of congenital heart disease. In this defect, there is no pulmonary valve opening and there is a ventricular septal defect. In these cases, the right ventricle is often an adequate size. Children with this condition often also have major aortopulmonary collaterals, which are extra arteries bringing blood to the lungs from the aorta.
Pulmonary atresia with ventricular septal defect is common in a syndrome called DiGeorge syndrome, also known as 22q11.2 deletion syndrome, and most children with this type of congenital heart disease are checked for that syndrome.
How is it treated?
Most children with pulmonary atresia with a ventricular septal defect require a heart catheterization or heart surgery. Often a heart catheterization is recommended to evaluate for major aortopulmonary collaterals. In some cases during catheterization, the valve may be opened.
Sometimes a pulmonary conduit may be placed surgically. In many cases a staged surgical approach is the best choice for this condition.
PULMONARY HYPERTENSION
What is pulmonary hypertension?
Pulmonary hypertension is a condition in which the pressure in the lung arteries is higher than normal. This can be difficult to diagnose. When you have your blood pressure checked in your arms or legs, this is systemic blood pressure. The lung blood pressure is much more difficult to check. An electrocardiogram and echocardiogram can help to diagnose pulmonary hypertension.
There are multiple causes of pulmonary hypertension:
- Congenital heart disease
- Mitral stenosis
- Pulmonary vein abnormalities
- Obstructive sleep apnea
- Unknown causes
Symptoms of pulmonary hypertension include shortness of breath, difficulty with exercise and, in younger children, difficulty growing.
How is it treated?
A heart catheterization is often recommended to directly measure pressure in the right ventricle and the arteries going to the lungs. During the heart catheterization, medications may be given to see if they change these pressures. Treatment depends on the findings in the heart catheterization and whether symptoms are improved.
PULMONARY REGURGITATION
What is pulmonary regurgitation?
The pulmonary valve is the valve between the right ventricle and the pulmonary artery. This is the valve that opens when the right ventricle pumps deoxygenated blood to the lungs in order to be oxygenated. The pulmonary valve usually has trivial regurgitation (leakage).
Pulmonary regurgitation is abnormal leaking of the pulmonary valve. This can be present at birth or develop over time. Some children have pulmonary regurgitation after surgery for congenital heart disease.
How is it treated?
If your child has pulmonary regurgitation, an echocardiogram will be done to evaluate whether the leaking is mild, moderate or severe. A cardiac MRI may be recommended to evaluate the size of the right ventricle. Pulmonary regurgitation can lead to right ventricular enlargement. An exercise study also may be needed.
Your cardiologist will discuss any symptoms your child may have, including chest pain, dizziness, fainting or palpitations.
If the leaking is severe, if the right ventricle is too large, if the exercise study is abnormal or if your child has symptoms, a heart catheterization or heart surgery may be recommended.
PULMONARY STENOSIS
What is pulmonary stenosis?
The pulmonary valve is the valve between the right ventricle and the pulmonary artery. This is the valve that opens when the right ventricle pumps deoxygenated blood to the lungs in order to be oxygenated. Pulmonary stenosis is an abnormal narrowing of the valve. This can be present at birth or develop over time. Pulmonary stenosis is common in a syndrome called Noonan syndrome.
How is it treated?
If your child has pulmonary stenosis, an echocardiogram will be done to evaluate whether the narrowing is mild, moderate or severe. An exercise study also may be needed.
Your cardiologist will discuss any symptoms your child may have, including chest pain, dizziness, fainting or palpitations.
If the pulmonary stenosis is severe, if the exercise study is abnormal or if your child has symptoms, a heart catheterization or heart surgery may be recommended.
RESTRICTIVE CARDIOMYOPATHY
What is restrictive cardiomyopathy?
Restrictive cardiomyopathy is the rarest type of cardiomyopathy in children. This occurs when the chambers of the heart become stiff and do not relax normally. It usually does not run in families.
How is it treated?
Restrictive cardiomyopathy can sometimes be treated with medications, including beta blockers, ACE inhibitors and diuretics. Sometimes children are restricted from sports for safety reasons. In cases of severe cardiomyopathy, some children require surgery or a heart transplant.
RHEUMATIC HEART DISEASE
What is rheumatic heart disease?
Rheumatic heart disease is the most common type of acquired heart disease in children in developing countries. Rheumatic heart disease usually occurs as a result of rheumatic fever caused by a group A streptococcal (strep) infection. This is the main reason for treating strep throat with antibiotics.
The major risk of acute rheumatic fever is fibrosis of the heart valves, most commonly the mitral or aortic valves. This can cause aortic regurgitation, aortic stenosis, mitral regurgitation, mitral stenosis or mitral valve prolapse.
How is it treated?
Acute rheumatic fever can be prevented by treating acute throat infections caused by group A streptococcus. Usually this requires 10 days of an oral antibiotic or a single intramuscular penicillin injection.
People who have had rheumatic fever are at high risk for a recurrent infection, which worsens the damage to the heart. If a child or teenager has rheumatic heart disease, they usually will require regular administration of antibiotics for many years.
Treatment of the heart valve disease in rheumatic heart disease depends on the specific valve affected and the severity of the valve disease.
SUBAORTIC MEMBRANE
What is a subaortic membrane?
The aortic valve is the valve between the left ventricle and the aorta. This is the valve that opens when the heart pumps blood out to the body.
A subaortic membrane is a rare type of congenital heart disease. With this condition, a shelflike membrane forms under the aortic valve.
Subaortic membranes are often diagnosed when a heart murmur is heard during a medical provider’s physical exam. Sometimes they are diagnosed incidentally when an echocardiogram is being done for another reason.
Some people with subaortic membranes never have any problems. In some cases, these membranes can cause the aortic valve to have problems over time. People with subaortic membranes can develop aortic stenosis or aortic regurgitation.
How is it treated?
People with subaortic membranes should be seen by a cardiologist. In some cases, no treatment is required. In other cases, if there is aortic stenosis or aortic regurgitation, a heart catheterization or surgery may be required.
SUPRAVENTRICULAR TACHYCARDIA
What is supraventricular tachycardia?
Supraventricular tachycardia is a fast heart rhythm coming from the upper chambers of the heart. There are multiple types of supraventricular tachycardia:
- Sinus tachycardia
- Atrial tachycardia
- Re-entrant tachycardia
- Junctional ectopic tachycardia
- Atrial flutter
- Atrial fibrillation
Usually when people say “supraventricular tachycardia,” they are referring to the re-entrant type. The most common causes of this in children is either an extra electrical pathway in the heart (Wolff-Parkinson-White syndrome is one cause of this) or an abnormality called atrioventricular nodal re-entrant tachycardia.
People with supraventricular tachycardia often have palpitations, which is a sensation of the heart going too fast. Sometimes they also have chest pain, dizziness, lightheadedness or fainting. If your child feels faint, actually faints or has chest pain with supraventricular tachycardia, it is important to seek care immediately.
Atrial flutter is rare in children, but it can occur in babies before or after birth. Atrial flutter also can happen in children with congenital heart disease. Atrial fibrillation is quite rare in children.
How is it treated?
In cases of re-entrant tachycardia, there are options for treatment:
- Medications such as beta blockers
- Electrophysiology study with possible ablation
No treatment is sometimes an option, especially if the tachycardia does not happen very often.
If your child has supraventricular tachycardia, your cardiologist will discuss all of the above options. If your child has sinus tachycardia or atrial tachycardia, medications may be recommended, depending on symptoms and how often they occur.
SYNCOPE
See Fainting
TETRALOGY OF FALLOT
What is Tetralogy of Fallot?
Tetralogy of Fallot is a type of congenital heart disease. It includes four heart problems:
- A ventricular septal defect
- Pulmonary stenosis and other types of obstruction of blood flow from the right ventricle to the lungs
- An overriding aorta (the aorta comes from both ventricles instead of just the left ventricle)
- Right ventricular hypertrophy (an enlarged right side of the heart)
Tetralogy of Fallot is the most common complex congenital heart disease. It is often diagnosed before birth or just after birth. Pulse oximetry screening in the newborn nursery can help with diagnosis.
Most babies and children with tetralogy of Fallot are otherwise normal. Tetralogy of Fallot is common in a syndrome called DiGeorge syndrome, also known as 22q11.2 deletion syndrome, and some children with this type of congenital heart disease are checked for that syndrome.
How is it treated?
Most children with tetralogy of Fallot require heart surgery as babies, usually in the first year. Children with this disease will always require a cardiologist and may require other heart procedures later in life.
TOTAL ANOMALOUS PULMONARY VENOUS RETURN
What is total anomalous pulmonary venous return?
Total anomalous pulmonary venous return is a type of congenital heart disease.
In a normal heart, there are four pulmonary veins (two from the right lung and two from the left lung) that bring oxygenated blood back from the lungs to the left atrium, so that the oxygenated blood can be pumped out to the body.
In total anomalous pulmonary venous return, all of the pulmonary veins return to the wrong place. This is often diagnosed before birth or just after birth. Pulse oximetry screening in the newborn nursery can help to diagnose this.
How is it treated?
All children with total anomalous pulmonary venous return require heart surgery, often as newborns and usually in the first few months. Children with this condition will always require a cardiologist and may require other heart procedures later in life.
TRANSPOSITION OF THE GREAT ARTERIES
What is transposition of the great arteries?
Transposition of the great arteries is a type of congenital heart disease.
In a normal heart, the pulmonary artery comes from the right ventricle and the aorta comes from the left ventricle. In transposition of the great arteries, these arteries are switched so that the pulmonary artery comes from the left ventricle and the aorta comes from the right ventricle. This results in inefficient circulation.
This is often diagnosed before birth or just after birth. Pulse oximetry screening in the newborn nursery can help to diagnose this.
How is it treated?
All children with transposition of the great arteries require heart surgery, often as newborns and usually in the first few months. Children with this disease will always require a cardiologist and may require other heart procedures later in life.
TRICUSPID ATRESIA
What is tricuspid atresia?
The tricuspid valve is the valve between the right atrium and the right ventricle. This is the valve that opens when deoxygenated blood from the body is delivered to the right ventricle so that it can be pumped to the lungs in order to be oxygenated.
Tricuspid atresia is a type of congenital heart disease. In this defect, there is no tricuspid valve opening. The right ventricle is usually too small to function normally.
This is often diagnosed before birth or just after birth. Pulse oximetry screening in the newborn nursery can help to diagnose this.
How is it treated?
Most children with tricuspid atresia require heart surgery in the first few months. In most cases a staged surgical approach is the best choice for tricuspid atresia. This usually consists of at least three heart surgeries in early childhood.
TRICUSPID REGURGITATION
What is tricuspid regurgitation?
The tricuspid valve is the valve between the right atrium and the right ventricle. This is the valve that opens when deoxygenated blood from the body is delivered to the right ventricle so that it can be pumped to the lungs in order to be oxygenated. The tricuspid valve normally leaks a trivial amount.
Tricuspid regurgitation is abnormal leaking of the tricuspid valve. This can be present at birth or develop over time. Tricuspid regurgitation is common in Ebstein’s anomaly, pulmonary hypertension and some other types of congenital heart disease. People with cardiomyopathy also may have tricuspid regurgitation.
How is it treated?
If your child has tricuspid regurgitation, an echocardiogram will be done to evaluate whether the leaking is mild, moderate or severe. Your cardiologist will discuss any symptoms your child may have, including chest pain, dizziness, fainting or palpitations.
If the leaking is severe, if other parts of the heart are changing as a result of the leaking or if your child has symptoms, he or she may need surgery.
TRICUSPID STENOSIS
What is tricuspid stenosis?
The tricuspid valve is the valve between the right atrium and the right ventricle. This is the valve that opens when deoxygenated blood from the body is delivered to the right ventricle so that it can be pumped to the lungs in order to be oxygenated.
Tricuspid stenosis is an abnormal narrowing of this valve. This can be present at birth or develop over time. Tricuspid stenosis is extremely rare.
How is it treated?
If your child has tricuspid stenosis, an echocardiogram will be done to evaluate whether the narrowing is mild, moderate or severe. An exercise study may also be needed. Your cardiologist will discuss any symptoms your child may have, including chest pain, dizziness, fainting or palpitations.
If the tricuspid stenosis is severe, if the exercise study is abnormal or if your child has symptoms, the treatment is surgery or a heart catheterization.
TRUNCUS ARTERIOSUS
What is truncus arteriosus?
Truncus arteriosus is a type of congenital heart disease.
In a normal heart, the pulmonary artery comes from the right ventricle and the aorta comes from the left ventricle. In truncus arteriosus, there is just one big artery that is a combination of the aorta and the pulmonary artery. This is extremely rare.
This is often diagnosed before birth or just after birth. Pulse oximetry screening in the newborn nursery can help to diagnose this.
Truncus arteriosus is common in a syndrome called DiGeorge syndrome, also known as 22q11.2 deletion syndrome, and many children with this type of congenital heart disease are checked for that syndrome.
How is it treated?
All children with truncus arteriosus require heart surgery, often as newborns and usually in the first few months. Children with truncus arteriosus will always require a cardiologist and may require other heart procedures later in life.
VASCULAR RING
What is a vascular ring?
A vascular ring is an abnormality involving the aorta, the pulmonary arteries or the vessels coming off the aorta. In certain cases, a combination of arteries can cause a ring that presses on the esophagus, the trachea (the tube that goes to the lungs) or both.
Vascular rings are sometimes suspected if a child has frequent lung infections, difficulty swallowing or noisy breathing.
If a vascular ring is suspected, there are tests that can help in diagnosis. These include an echocardiogram, a barium swallow and a CT angiogram.
How is it treated?
If a vascular ring is found, surgery may be recommended to release the ring.
VENTRICULAR SEPTAL DEFECT
What is a ventricular septal defect?
A ventricular septal defect is a hole between the right and left ventricles, which are the two muscular pumping chambers of the heart.
Most children with a ventricular septal defect have no other problems. In some cases, there are other heart defects.
If your child is diagnosed with a ventricular septal defect, it will be categorized as one of the following:
- Perimembranous (also known as subarterial or membranous)
- Outlet (supracristal)
- Inlet
- Muscular
- Malalignment
The size will also be described as tiny, small, moderate restrictive, moderate unrestrictive or large.
How is it treated?
The treatment for a ventricular septal defect depends on the type and size.
Perimembranous or membranous ventricular septal defects often require treatment. If they are unrestrictive, surgery is often recommended in the first year. If perimembranous ventricular septal defects are small, cardiology follow-up is necessary to monitor the aortic valve.
The most common type is a muscular ventricular septal defect. Tiny and small muscular ventricular septal defects usually do not require treatment.
WOLFF-PARKINSON-WHITE SYNDROME
What is Wolff-Parkinson-White syndrome?
Wolff-Parkinson-White syndrome is a type of electrical abnormality in the heart.
The heart’s electrical system prompts the heart to contract and efficiently pump blood to the lungs and body. These electrical impulses begin in the upper chambers of the heart. In a normal heart, there is only one way for the electrical impulse to travel.
People with Wolff-Parkinson-White syndrome have an extra electrical pathway in the heart. They also are more likely to have supraventricular tachycardia.
People with Wolff-Parkinson-White syndrome can be at risk for dangerous heart rhythms. Rarely, people can have rate-dependent Wolff-Parkinson-White syndrome, in which their extra pathway is only apparent at certain heart rates.
Wolff-Parkinson-White syndrome often can be diagnosed with an electrocardiogram. The syndrome can run in families. If someone is diagnosed with this condition, an electrocardiogram is recommended for first-degree family members.
How is it treated?
Some people with Wolff-Parkinson-White syndrome never have supraventricular tachycardia. If your child is found to have Wolff-Parkinson-White syndrome, an echocardiogram may be done to evaluate for any congenital heart disease. A Holter monitor or event monitor may be recommended to evaluate for supraventricular tachycardia. An exercise study can help to determine whether the syndrome’s electrical pathway is safe or dangerous.
Treatment options may include:
- Medications such as beta blockers
- Electrophysiology study with possible ablation
No treatment is sometimes an option, especially if the supraventricular tachycardia does not happen very often and an exercise study has shown the electrical pathway to be safe.
If your child has supraventricular tachycardia, your cardiologist will discuss all of the above options.
Meet Our Team
Contact Us
Logan Health Heart & Lung
350 Heritage Way, Suite 2100
Kalispell, MT 59901
Phone: (406) 257-8992
Fax: (406) 257-8996
Hours: Monday through Friday 8 a.m. to 5 p.m.